[DISCLAIMER: This answer presumes there is no collective bargaining agreement or landlord/municipal host terms that impact the library's flexibility while revising their Safety Plan.]
Okay, with that disclaimer out of the way, here are my "short answers" to these excellent questions:
"[F]or those in shared offices, how do we handle the vaccinated/not vaccinated issue?"
Short answer: Revise your library's current Safety Plan to specify how it has adopted the 5/19 NY Forward Guidelines (for advice on how to do that, please see my "Long Answer," below).
"Do we go with the honor system and tell those in shared offices that if they are vaccinated, they may go maskless?"
Short answer: I advise requiring proof (for the legal/operational rationale behind this opinion, please see my "Long Answer," below).
"I've heard that some restaurants are allowing their servers to go maskless if they show proof of their vaccination to their employer. Would we be allowed to do something like that?"
Short answer: Yes (for more on that, please see my "Long Answer", below!).
Long Answer
This question comes at a good time, since on June 10, 2021, the U.S. Occupational Safety & Hazard Administration ("OSHA") updated its guidance for employers on protecting workers from COVID-19.[1] This new "6/10 OSHA Guidance" speaks to questions like these.
But first, a quick recap.
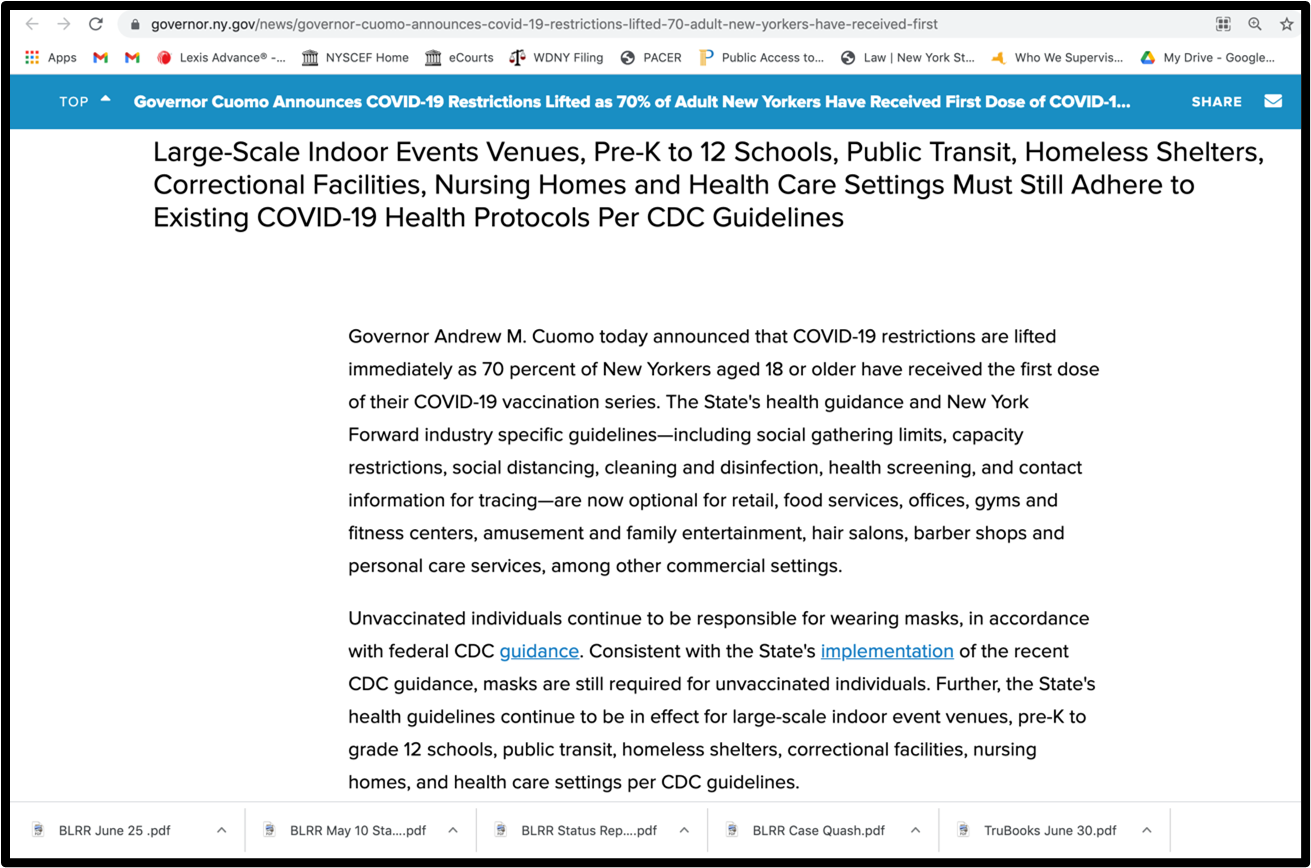
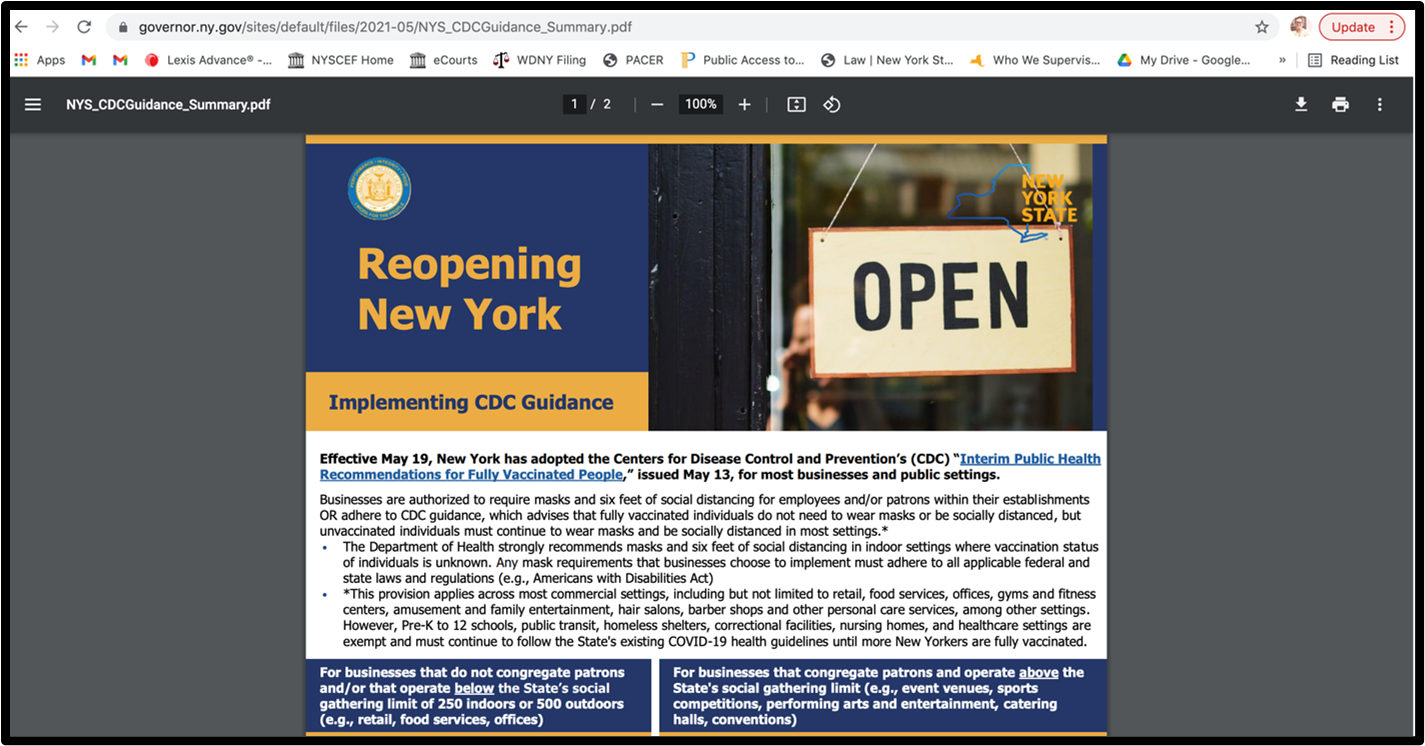
When the CDC came out with their "surprise" interim guidance for fully vaccinated people on May 13th, 2021 (the "5/13 CDC Guidance"), it took New York six days to incorporate it (into the "5/19 NY Guidance").
OSHA, on the other hand, took a bit more than six days.[2] But by June 10th, here's what they had to say:
CDC's Interim Public Health Recommendations for Fully Vaccinated People explain that under most circumstances, fully vaccinated people need not take all the precautions that unvaccinated people should take. For example, CDC advises that most fully vaccinated people can resume activities without wearing masks or physically distancing, except where required by federal, state, local, tribal, or territorial laws, rules and regulations, including local business and workplace guidance.
And from there, OSHA takes it granular.[3]
The 6/10 OSHA Guidance sets out an array of factors for employers and workers to not just consider in isolation, but to think about as a continuum of risk assessment and safety measures. The factors they list include consideration of vaccination status, and shared office space.
Because it is so critical that employers get this right, I am putting this "6/10 OSHA Guidance"[4] below. Now that we have this resource, I strongly advise employers to refer to it when updating their Safety Plan to include the 5/19 NY Guidance.
And now, for this library's very specific set of questions about non-public, shared office space, here is the rest of my "long answer."
As you can see in OSHA's listing, the consideration of shared office space isn't simply one of vaccination and proximity. It also involves the consideration of things such as ventilation, worker education, and individual worker vulnerabilities.
Because of this, there is no "one size fits all" answer to this library's question. Rather, the library should review the non-public, shared workspace against the OSHA criteria, and then craft a customized plan...recognizing that the protocol for areas with up-to-date HVAC systems will be different from a work area near the stacks where there might be very little fresh air.
This variability is the key consideration of shared non-public workspace. Your library's safety measures may be different when the weather is cold and workers can't open a window. Your library's Safety Plan measures may be limited if the workspace is near a rare book collection or other assets requiring precise climate control. And on top of that (literally, as an add-on after the fact) your library will need to consider the impact that a Safety Plan's working conditions can have on individuals with disclosed, pre-existing conditions (such as allergies, heightened vulnerability to COVID, or a health condition impeding vaccination).[5]
Within all this variability (which is a LOT for any employer to handle, to say nothing of a library that is also focusing most of its energy on meeting the needs of the public), I advise requesting proof of vaccination for two reasons. First, it positions an employer to be more confident in their adherence to the plan they develop. Second, it positions employees to be confident that they are in a position to advocate for their own health.
Now, on the flip side, the employee relations challenge of requiring workers to provide vaccination status can be onerous. Some people are just not comfortable revealing that type of information, and I totally get it. BUT the EEOC and the New York State Division of Human Rights have both determined that an employer requesting proof of vaccination is not the same as an employer demanding disclosure of confidential medical information.[6] Barring a union contract or other term forbidding the demanding proof of vaccination, employers should be confident they can require it.
That confidence can, in turn, transfer to the employees who are certain that their unmasked and nearby co-workers are vaccinated. In my experience, nothing can erode trust like an honor system where someone is suspected of being dishonorable. Further, that suspicion can turn into full-on blame if a worst-case scenario emerges and someone does get sick.
And while the current CDC and NY Forward guidance mean an employer won't likely be successfully sued for using the honor system as opposed to requiring proof, I wouldn't put it past one of my fellow attorneys to try.[7] This is especially true if your library's Safety Plan or past planning has identified certain front-facing work or other tasks as "higher" risk, meaning there is an acknowledgement on the record that some work may bring increased exposure.
Okay, to sum up: you don't have to, but it's worth considering requiring proof of vaccination. But most critically, whatever your library does, if you update your Safety Plan, factor in the new 6/10 OSHA Guidance.
Since the combination of options is extensive (New guidance? Old? Require vaccinations? Proof?) I have laid out a chart below. Below that are some of the high points of the 6/10 OSHA Guidance, which every employer should read.
I hope this reply makes up for in helpfulness what it poses in complexity. I wish you calm and careful planning as your library moves into this next phase.
|
Safety Plan -->
Employee requirement -->
|
No Use of NY Forward 5/19 guidance[8]
|
Updated to NY Forward 5/19 guidance
and uses "honor system" only for employees
|
Updated to NY 5/19 guidance and library requires proof of
vaccination for employees
|
|
Employee vaccination status not considered in Safety Plan
|
This means your library is still using your pre-May 19th Safety Plan; that's fine, just stick to it until it is updated.
|
Not possible (if using 5/19 guidance, the library must consider vaccination status).
|
Not possible (if using 5/19 guidance, the library must consider vaccination status).
|
|
Employee vaccination status considered in Safety Plan but vaccination is not required to perform routine duties of job
|
This means your library is still using your pre-May 19th Safety Plan; that's fine, just stick to it until it is updated.
|
If your library is using the honor system, but still structured so vaccination is not a factor in performance of routine duties, so long as the OSHA 6/10 guidance doesn't suggest otherwise, carry on!
|
If your library is requiring proof of vaccination to use 5/19 guidelines, but still structured so vaccination is not a factor in performance of routine duties, so long as the OSHA 6/10 guidance doesn't suggest otherwise, carry on!
|
|
Library-employer requires vaccination as part of Safety Plan and vaccination is required to perform routine duties of job.
|
With such rigorous requirements, assessing the Safety Plan under the OSHA 6/10/21 guidance is wise.
|
This combination brings some risk since it bases safety on vaccination but does not require proof, which limits the ability to assuage employee relations concerns regarding unvaccinated colleagues.
|
This combination provides the best documentation of maximum risk management and positions library to address employee relations concerns regarding unvaccinated colleagues.
|
|
OSHA
Except for workplace settings covered by OSHA's ETS and mask requirements for public transportation, most employers no longer need to take steps to protect their workers from COVID-19 exposure in any workplace, or well-defined portions of a workplace, where all employees are fully vaccinated. Employers should still take steps to protect unvaccinated or otherwise at-risk workers in their workplaces, or well-defined portions of workplaces. 2
Employers should engage with workers and their representatives to determine how to implement multi-layered interventions to protect unvaccinated or otherwise at-risk workers and mitigate the spread of COVID-19, including:
- Grant paid time off for employees to get vaccinated. The Department of Labor and OSHA, as well as other federal agencies, are working diligently to ensure access to COVID-19 vaccinations. CDC provides information on the benefits and safety of vaccinations. Businesses with fewer than 500 employees may be eligible for tax credits under the American Rescue Plan if they provide paid time off for employees who decide to receive the vaccine and to recover from any potential side effects from the vaccine.
- Instruct any workers who are infected, unvaccinated workers who have had close contact with someone who tested positive for SARS-CoV-2, and all workers with COVID-19 symptoms to stay home from work to prevent or reduce the risk of transmission of the virus that causes COVID-19. Ensure that absence policies are non-punitive. Eliminate or revise policies that encourage workers to come to work sick or when unvaccinated workers have been exposed to COVID-19. Businesses with fewer than 500 employees may be eligible for refundable tax credits under the American Rescue Plan if they provide paid time off for sick and family leave to their employees due to COVID-19 related reasons. The ARP tax credits are available to eligible employers that pay sick and family leave for qualified leave from April 1, 2021, through September 30, 2021. More information is available from the IRS.
- Implement physical distancing for unvaccinated and otherwise at-risk workers in all communal work areas. A key way to protect unvaccinated or otherwise at-risk workers is to physically distance them from other unvaccinated or otherwise at-risk people (workers or customers) – generally at least 6 feet of distance is recommended, although this is not a guarantee of safety, especially in enclosed or poorly ventilated spaces.
Employers could also limit the number of unvaccinated or otherwise at-risk workers in one place at any given time, for example by implementing flexible worksites (e.g., telework); implementing flexible work hours (e.g., rotate or stagger shifts to limit the number of such workers in the workplace at the same time); delivering services remotely (e.g., phone, video, or web); or implementing flexible meeting and travel options, all for such workers.
At fixed workstations where unvaccinated or otherwise at-risk workers are not able to remain at least 6 feet away from other people, transparent shields or other solid barriers (e.g., fire resistant plastic sheeting or flexible strip curtains) can separate these workers from other people. Barriers should block face-to-face pathways between individuals in order to prevent direct transmission of respiratory droplets, and any openings should be placed at the bottom and made as small as possible. The posture (sitting or standing) of users and the safety of the work environment should be considered when designing and installing barriers, as should the need for enhanced ventilation.
- Provide unvaccinated and otherwise at-risk workers with face coverings or surgical masks, unless their work task requires a respirator or other PPE. Such workers should wear a face covering that covers the nose and mouth to contain the wearer's respiratory droplets and help protect others and potentially themselves. Face coverings should be made of at least two layers of a tightly woven breathable fabric, such as cotton, and should not have exhalation valves or vents. They should fit snugly over the nose, mouth, and chin with no large gaps on the outside of the face. CDC provides general guidance on masks.
Employers should provide face coverings to unvaccinated and otherwise at-risk workers at no cost. Under federal anti-discrimination laws, employers may need to provide reasonable accommodation for any workers who are unable to wear or have difficulty wearing certain types of face coverings due to a disability or who need a religious accommodation under Title VII. In workplaces with employees who are deaf or hard of hearing, employers should consider acquiring masks with clear coverings over the mouth for unvaccinated and otherwise at-risk workers to facilitate lip-reading.
Unless otherwise provided by federal, state, or local requirements, unvaccinated workers who are outdoors may opt not to wear face coverings unless they are at-risk, for example, if they are immunocompromised. Regardless, all workers should be supported in continuing face covering use if they choose, especially in order to safely work closely with other people.
When an employer determines that PPE is necessary to protect unvaccinated and otherwise at-risk workers, the employer must provide PPE in accordance with relevant mandatory OSHA standards and should consider providing PPE in accordance with other industry-specific guidance. Respirators, if necessary, must be provided and used in compliance with 29 CFR 1910.134 (e.g., medical determination, fit testing, training on its correct use), including certain provisions for voluntary use when workers supply their own respirators, and other PPE must be provided and used in accordance with the applicable standards in 29 CFR 1910, Subpart I (e.g., 1910.132 and 133). There are times when PPE is not called for by OSHA standards or other industry-specific guidance, but some workers may have a legal right to PPE as a reasonable accommodation under the ADA. Employers are encouraged to proactively inform employees who have a legal right to PPE as a reasonable accommodation for their disability about how to make such a request. Other workers may want to use PPE if they are still concerned about their personal safety (e.g., if a family member is at higher-risk for severe illness, they may want to wear a face shield in addition to a face covering as an added layer of protection). Encourage and support voluntary use of PPE in these circumstances and ensure the equipment is adequate to protect the worker.
For operations where the face covering can become wet and soiled, provide unvaccinated and otherwise at-risk workers with replacements daily or more frequently, as needed. Face shields may be provided for use with face coverings to protect them from getting wet and soiled, but they do not provide protection by themselves. See CDC's Guide to Masks.
Employers with workers in a setting where face coverings may increase the risk of heat-related illness indoors or outdoors or cause safety concerns due to introduction of a hazard (for instance, straps getting caught in machinery) may wish to consult with an occupational safety and health professional to help determine the appropriate face covering/respirator use for their setting.
- Educate and train workers on your COVID-19 policies and procedures using accessible formats and in language they understand. Train managers on how to implement COVID-19 policies. Communicate supportive workplace policies clearly, frequently, and via multiple methods to promote a safe and healthy workplace. Communications should be in plain language that unvaccinated and otherwise at-risk workers understand (including non-English languages, and American Sign Language or other accessible communication methods, if applicable) and in a manner accessible to individuals with disabilities. Training should be directed at employees, contractors, and any other individuals on site, as appropriate, and should include:
- Basic facts about COVID-19, including how it is spread and the importance of physical distancing (including remote work), ventilation, vaccination, use of face coverings, and hand hygiene.
- Workplace policies and procedures implemented to protect workers from COVID-19 hazards.
For basic facts, see About COVID-19 and What Workers Need to Know About COVID-19, above and see more on vaccinations, improving ventilation, physical distancing (including remote work), PPE, and face coverings, respectively, elsewhere in this document. Some means of tracking which workers have received this information, and when, could be utilized, by the employer, as appropriate.
In addition, ensure that workers understand their rights to a safe and healthful work environment, whom to contact with questions or concerns about workplace safety and health, and their right to raise workplace safety and health concerns free from retaliation. This information should also be provided in a language that workers understand. (See Implementing Protections from Retaliation, below.) Ensure supervisors are familiar with workplace flexibilities and other human resources policies and procedures.
- Suggest that unvaccinated customers, visitors, or guests wear face coverings, especially in public-facing workplaces such as retail establishments, if there are unvaccinated or otherwise at-risk workers in the workplace who are likely to interact with these customers, visitors, or guests. This could include posting a notice or otherwise suggesting unvaccinated people wear face coverings, even if no longer required by your jurisdiction. Individuals who are under the age of 2 or are actively consuming food or beverages on site need not wear face coverings.
- Maintain Ventilation Systems. The virus that causes COVID-19 spreads between people more readily indoors than outdoors. Improving ventilation is a key engineering control that can be used as part of a layered strategy to reduce the concentration of viral particles in indoor air and the risk of virus transmission to unvaccinated workers in particular. Some measures to improve ventilation are discussed in CDC's Ventilation in Buildings and in the OSHA Alert: COVID-19 Guidance on Ventilation in the Workplace. These recommendations are based on ASHRAE Guidance for Building Operations During the COVID-19 Pandemic. Adequate ventilation will protect all people in a closed space. Key measures include ensuring the HVAC system(s) is operating in accordance with the manufacturer's instructions and design specifications, conducting all regularly scheduled inspections and maintenance procedures, maximizing the amount of outside air supplied, installing air filters with a Minimum Efficiency Reporting Value (MERV) 13 or higher where feasible, maximizing natural ventilation in buildings without HVAC systems by opening windows or doors, when conditions allow (if that does not pose a safety risk), and considering the use of portable air cleaners with High Efficiency Particulate Air (HEPA) filters in spaces with high occupancy or limited ventilation.
- Perform routine cleaning and disinfection. If someone who has been in the facility within 24 hours is suspected of having or confirmed to have COVID-19, follow the CDC cleaning and disinfection recommendations. Follow requirements in mandatory OSHA standards 29 CFR 1910.1200 and 1910.132, 133, and 138 for hazard communication and PPE appropriate for exposure to cleaning chemicals.
- Record and report COVID-19 infections and deaths: Under mandatory OSHA rules in 29 CFR 1904, employers are responsible for recording work-related cases of COVID-19 illness on OSHA's Form 300 logs if the following requirements are met: (1) the case is a confirmed case of COVID-19; (2) the case is work-related (as defined by 29 CFR 1904.5); and (3) the case involves one or more relevant recording criteria (set forth in 29 CFR 1904.7) (e.g., medical treatment, days away from work). Employers must follow the requirements in 29 CFR 1904 when reporting COVID-19 fatalities and hospitalizations to OSHA. More information is available on OSHA's website. Employers should also report outbreaks to health departments as required and support their contact tracing efforts.
In addition, employers should be aware that Section 11(c) of the Act prohibits reprisal or discrimination against an employee for speaking out about unsafe working conditions or reporting an infection or exposure to COVID-19 to an employer. In addition, mandatory OSHA standard 29 CFR 1904.35(b) also prohibits discrimination against an employee for reporting a work-related illness.
Note on recording adverse reactions to vaccines: DOL and OSHA, as well as other federal agencies, are working diligently to encourage COVID-19 vaccinations. OSHA does not want to give any suggestion of discouraging workers from receiving COVID-19 vaccination or to disincentivize employers' vaccination efforts. As a result, OSHA will not enforce 29 CFR 1904's recording requirements to require any employers to record worker side effects from COVID-19 vaccination through May 2022. OSHA will reevaluate the agency's position at that time to determine the best course of action moving forward. Individuals may choose to submit adverse reactions to the federal Vaccine Adverse Event Reporting System.
- Implement protections from retaliation and set up an anonymous process for workers to voice concerns about COVID-19-related hazards: Section 11(c) of the OSH Act prohibits discharging or in any other way discriminating against an employee for engaging in various occupational safety and health activities. Examples of violations of Section 11(c) could include discriminating against employees for raising a reasonable concern about infection control related to COVID-19 to the employer, the employer's agent, other employees, a government agency, or to the public, such as through print, online, social, or any other media; or against an employee for voluntarily providing and safely wearing their own PPE, such as a respirator, face shield, gloves, or surgical mask.
In addition to notifying workers of their rights to a safe and healthful work environment, ensure that workers know whom to contact with questions or concerns about workplace safety and health, and that there are prohibitions against retaliation for raising workplace safety and health concerns or engaging in other protected occupational safety and health activities (see educating and training workers about COVID-19 policies and procedures, above); also consider using a hotline or other method for workers to voice concerns anonymously.
- Follow other applicable mandatory OSHA standards: All of OSHA's standards that apply to protecting workers from infection remain in place. These mandatory OSHA standards include: requirements for PPE (29 CFR 1910, Subpart I (e.g., 1910.132 and 133)), respiratory protection (29 CFR 1910.134), sanitation (29 CFR 1910.141), protection from bloodborne pathogens: (29 CFR 1910.1030), and OSHA's requirements for employee access to medical and exposure records (29 CFR 1910.1020). Many healthcare workplaces will be covered by the mandatory OSHA COVID-19 Emergency Temporary Standard. More information on that standard is available on the OSHA website at [link]. Where the ETS does not apply, employers are required under the General Duty Clause, Section 5(a)(1) of the OSH Act, to provide a safe and healthful workplace free from recognized hazards that are causing or likely to cause death or serious physical harm .
Appendix: Measures Appropriate for Higher-Risk Workplaces with Mixed-Vaccination Status Workers
Employers should take additional steps to mitigate the spread of COVID-19 for unvaccinated and otherwise at-risk workers in workplaces where there is heightened risk due to the following types of factors:
- Close contact– where unvaccinated or otherwise at-risk workers are working close to one another, for example, on production or assembly lines. Such workers may also be near one another at other times, such as when clocking in or out, during breaks, or in locker/changing rooms.
- Duration of contact – where unvaccinated or otherwise at-risk workers often have prolonged closeness to coworkers (e.g., for 8–12 hours per shift). Continued contact with potentially infectious individuals increases the risk of SARS-CoV-2 transmission.
- Type of contact – unvaccinated or otherwise at-risk workers who may be exposed to the infectious virus through respiratory droplets in the air—for example, when unvaccinated or otherwise at-risk workers in a manufacturing or factory setting who have the virus cough or sneeze. It is also possible that exposure could occur from contact with contaminated surfaces or objects, such as tools, workstations, or break room tables. Shared spaces such as break rooms, locker rooms, and entrances/exits to the facility may contribute to their risk.
- Other distinctive factors that may increase risk among these unvaccinated or otherwise at-risk workers include:
- A common practice at some workplaces of sharing employer-provided transportation such as ride-share vans or shuttle vehicles;
- Frequent contact with other unvaccinated or otherwise at-risk individuals in community settings in areas where there is elevated community transmission; and
- Communal housing or living quarters onboard vessels with other unvaccinated or otherwise at-risk individuals.
In these types of higher-risk workplaces – which include manufacturing, meat and poultry processing, high-volume retail and grocery, and seafood processing – this Appendix provides best practices to protect unvaccinated or otherwise at-risk workers. Please note that these recommendations are in addition to those in the general precautions described above, including isolation of infected or possibly infected workers, and other precautions.
In all higher-risk workplaces where there are unvaccinated or otherwise at-risk workers:
- Stagger break times in these generally high-population workplaces, or provide temporary break areas and restrooms to avoid groups of unvaccinated or otherwise at-risk workers congregating during breaks. Unvaccinated or otherwise at-risk workers should maintain at least 6 feet of distance from others at all times, including on breaks.
- Stagger workers' arrival and departure times to avoid congregations of unvaccinated or otherwise at-risk in parking areas, locker rooms, and near time clocks.
- Provide visual cues (e.g., floor markings, signs) as a reminder to maintain physical distancing.
- Implement strategies (tailored to your workplace) to improve ventilation that protects workers as outlined in CDC's Ventilation in Buildings and in the OSHA Alert: COVID-19 Guidance on Ventilation in the Workplace.
In workplaces (or well-defined work areas) with processing or assembly lines where there are unvaccinated or otherwise at-risk workers:
- Working on food processing or assembly lines can result in virus exposure because these workplaces have often been designed for a number of workers to stand next to or across from each other to maximize productivity. Proper spacing of unvaccinated or otherwise at-risk workers (or if not possible, appropriate use of barriers) can help reduce the risks for such workers.
In retail workplaces (or well-defined work areas within retail) where there are unvaccinated or otherwise at-risk workers:
- Suggest masks for unvaccinated (or unknown-status) customers and other visitors.
- Consider means for physical distancing from other people who are not known to be fully vaccinated. If distancing is not possible, consider the use of barriers between work stations used by unvaccinated or otherwise at-risk workers and the locations customers will stand, with pass-through openings at the bottom, if possible.
- Move the electronic payment terminal/credit card reader farther away from any unvaccinated or otherwise at-risk workers in order to increase the distance between customers and such workers, if possible.
- Shift primary stocking activities of unvaccinated or otherwise at-risk workers to off-peak or after hours when possible to reduce contact between unvaccinated or otherwise at-risk workers and customers.
Unvaccinated and otherwise at-risk workers are also at risk when traveling to and from work in employer-provided buses and vans.
- Notify unvaccinated and otherwise at-risk workers of this risk and, to the extent feasible, help them limit the number of such workers in one vehicle.
- Make sure all unvaccinated and otherwise at-risk workers sharing a vehicle are wearing appropriate face coverings.
[1] While not every library is covered by OSHA regulations, OSHA's standards are a "go-to" for protecting workers, and much of New York's guidance on COVID safety refers employers to their materials.
[2] Considering what's at stake, I appreciate that.
[3] "Granular:" a tired buzzword, I know. What word/phrase would I have used pre-2014? "Particular?" "Minutely specific?" Look at all that CDC minutia! Sometimes "granular" really does get the job done.
[4] Found at https://www.osha.gov/coronavirus/safework as of June 14th, 2021.
[5] I once worked in a dampish half-basement that had a window that would open onto a thriving crop of ragweed. In the winter, the mold from the damp got activated by the heating units. Hello, allergies!
[6]https://www.eeoc.gov/wysk/what-you-should-know-about-covid-19-and-ada-rehabilitation-act-and-other-eeo-laws
[7] This is how the law changes, after all.
[8] This means no relaxing of social distancing and face-covering rules; they are at pre-May 19th levels.covid